Acute Renal Failure (ARF) - "The Kopp Solution"
Acute Renal Failure (ARF) – "The Kopp Solution". Obviously the title of this paper offers a twofold interpretation. First, the author's clinical solution how to recognize, prevent and how to conservatively treat ARF is described. Second, the solution of the problem has also led to the development of a special intravenous solution which is basically needed to provide the ideal qualitative and quantitative substrate for the kidney to survive the toxic or ischemic injury leading to ARF. Finally, in our experience, the routine use of the newly developed protocol of Bicarbonate-Alkaline-Polyuria (BAP) for all the risk groups defined below has led to a significant decrease of ARF in need of dialysis resulting in a greater number of patients who survive ARF conservatively and lastly to an increased number of vital, polyuric kidneys useful for transplantation.
Keywords: Acute-Renal-Failure – “The Kopp Solution”
The clinical situation of Acute Renal Failure (ARF) is characterized by an unproportionate socio-economic burden and high costs which are due to the frequent development of ARF into the so- called Multi-Organ-Failure (MOF). The mortality rate of MOV is at minimum 50% (23, 24). To date, only artificial and highly cost intensive remedy is offered by extracorporeal blood-purification-techniques. The recent ARF-Satellite-Symposion of ISN in May 1999 in Chile has confirmed that the worldwide medical research and experimental efforts on the molecular and cellular level have as yet NOT led to a breakthrough (8). However, we were able to find a clinical solution to this problem on a clinical and patho-physiological basis. We developed and applied clinically on patients a special type of DIURESIS, the so called BICARBONATE-ALCALINE-POLYURIA (BAP) (9, 10, 11).
At first, It is very important to primarily evaluate the RISK of a patient to develop ARF. Unfortunately not only in Nephrology but also in many other disciplines the RISK regarding the occurence of ARF with the need of dialysis is grossly underestimated, although it constitutes a life-threatening complication whatever the basic illness or trauma may be. Various exemples may be mentioned e.g. interventional and surgical Cardiology, Oncology, Geriatric Surgery and many others (2, 12, 13). A RISK-Score of 10 Patient-Groups with highly increased RISK to develop ARF is therefore presented first.
- Pre-existing Chronic Renal Insufficiency (CRI), Creatinine -> 1,6 mg/dl
- Age over 60 Years
- Dabetics I and II and Patients with Systemic Diseases
- Patients with only ONE Kidney, either functional or anatomic
- Nephrotoxins, exogen: e.g. Aethylenglycol, Tetracarbonchloride, Herbicides, Mushroms etc.
- Nephrotoxins, endogenous: eg. Sepsis, Rhabdomyolysis, Haemolysis, Hyperuricemia, Oxalosis etc.
- Electrolyte-Fluid-Acid-Base-derangements, e.g. Dehydration, Drainages, Diarrhoe, etc.
- Pregnancy with Risk of EPH, HELLP, and other Chronic Renal Insufficiency (CRI)
- All Risks 1 – 8 pre- peri- and post-op large Interventions or pre- peri- post-interventions of intra-arterial or intra-venous Contrast-Media.
- All Risks 1 - 8 pre- peri and post Nephrotoxic Pharmaceuticals, e.g NSAIDs, Antibiotics, Cytostatic or Immunsupressive Drugs
Obviously, almost 70 % to 80 % o all patients of any large hospital will belong to those 10 categories. However, the most frequent cause of ARF is the underestimation of the risk of ARF to occur (5).
Therefore, the above list of RISKS is also the list oF INDICATIONS requiring early and effective prophylactic and therapeutic measures. The introduction and maintenance of the so called Bicarbonate-Alcaline-Polyuria (BAP) regimen is therefore mandatory.
At first, the EMERGENCY-PROCEDURE to produce BAP will be described. It should always be applied in all cases where the RISK for the development of ARF may not clearly be identified initially, e.g. myocardial infarction, trauma, shock etc. The EMERGENCY-PROCEDURE must always be carried out according to the rules and regulations of intensive care. (16, 18). It should be started routinely as early as possible as a means of “RENAL RESURRECTION” , together with a well trained nursing team, thus leading to favorable and encouraging results.
Emergency-Procedure I.V.
Blood-Gas Controls. Initially arterial, later after exclusion of hypoxia and hypercapnia > venous.
In order to over-correct or elevate the blood-bicarbonate-level to approx. 28 mMol/l = BE ~ +7
use 100 ml portions each of 1 Mol = 8,4 % NaHCO3 via Central Venous Access under ICU supervision.
Formula: 0,3 x bodyweight (kg) x (BE + 7 minus BE measured) = mMol or ml 1-molar NaHCO3
CAUTION: Cardio-pulmonary insufficiency, hypoxia, hypercapnia !!! Respirator therapy if indicated.
CAUTION: Alkaloses of other origin e.g. hypochloremia, hyperammonemia etc.
IMPORTANT: Na+, K+, Ca++, Cl- Correction to the normal !
Subsequent blood-gas-analyses may be venous.
AIM: Blood-BE > + 7 Then: loop-diuretic bolus I.V. : Dose: 40 mg Furosemide x Serum-Creatinine
AIM: Key-event: Urine pH > + 7.0 + Polyuria: > 125 ml/h = 2000 to 3000 ml/24h = BAP
Mandatory controls initially hourly, then 6 to 3 times daily: Urine-pH, Urine output, fluid balance, blood-gas-analysis, Electrolytes, Creatinine, BUN, Glucose (CAVE Diabetics); etc.
MAINTENANCE OF BAP is necessary until the kidney fully recovers > days or weeks !! (KOPP’s Solution if available)
LEADING PARAMETER is Urine-pH above +7.0
Note: The Kidney threshold for bicarbonate is variable and depends on numerous factors such as Volume, Potassium, Aldosterone etc. for any given patient. It can be as low as BE + 2 mMol/L. Therefore, repeated blood-gas and urine-pH-controls are needed in order to:
- To identify the lowest possible Blood-BE at which alkaline Urine-pH > +7.0 can be maintained.
- To prevent undesired systemic alkalosis.
Loop-diuretic Dose per 24 hrs: = identical to starting bolus = 40 mg Furosemide x Serum-Creatinine by continuous infusion, or alternatively Torasemide approx. ½ Dose of Furosemide
For a ~ 70 kg man Polyuria of 3000 to 4000 ml/ 24 hr/ is required in order
- to obtain adequate uremic waste clearances (diluted urine only)
- to obtain negative fluid balance, if required (e.g. fluid load by intravenous nutrition)
- to maintain normal serum levels Fluid and Electrolytes have to be precisely substituted
Note: Urine volumes of more than 6000 ml/24 hrs are possible and have to be managed
Elevated Serum-Creatinine will decrease by approx. 1 mg/dl daily after 1 or 2 days
Following the Emergency-Procedure I.V. practical clinical problems arise from the multitude of the many different I.V.-Infusions in different bottles which have to be administered at differing infusion-rates and with different compositions, thereby requiring multiple infusion-pumps.
In order to avoid these problems we were able to develop a single I.V.-Infusion-fluid the so-called Kopp’s-Solution which was prepared in the University- hospital pharmacy (TUM) on demand.
Its composition was as follows: Na+ 146 mMol/l; K+ 4 mMol/l; HCO -3 60mMol/l; Cl – 90 mMol/l.
With the use of this solution the continuous maintenance of the Bicarbonate-Alcaline-Polyuria was made simple and safe for the routine clinical practice. In preterminal, chronic renal
insufficiency, the retention of uremic waste-products was effectively treatable. Most likely, the efficacy of the Kopp’s Solution is based on its similarity with the physiological environment of sea-water in the DEVON-CARBON period.
Oral Prophylaxis
Early recognition of the risk of ARF, e.g. in planned interventions with antibiotics, contrast-media or cytotoxix drugs etc. will allow the oral introduction of Bicarbonate Alcaline Polyuria (BAP) within one or two days, using oral dosage forms, e.g. Tablets of Sodium-Bicarbonate and the oral administration of adequate amounts of fluids.
If POSSIBLE or AVAILBLE: BLOOD-GAS-ANALYSIS: Venous, Arterial in case of Hypoxia and/or Hypercapnia)
Oral Use of Gastro-resistant 100 mg Tablets Sodium hydrogen carbonate bicaNorm® (Fresenius Medical Care), Alka-Seltzer-Gold-effervescent-tablets, Sodium-hydrogen-carbonate tablets (Walgreen), Kaiser-Natron or any other NaHCO3 – Preparation available at drugstores either tablets or powder.
LEADING PARAMETER IS Urine-pH Optimum pH = 7,5 - 8,0
If Urine-pH is lower than pH 7.5 immediately take 3 tablets or 3 Gramms of NaHCO3 repeatedly until Urine-pH- Optimum is reached and continuously maintained.
There is no fixed Dose of NaHCO3 per day
If Creatinine is above 1,9 mg/dl (Patient 70 +/- 20 kg B.W.) use FUROSEMIDE- tablet 40 mg
Dose/ day = 40 mg x Serum Creatinine (or TORASEMIDE half of the Furosemide Dose) in order to enhance Urine-Flow up to >>125 ml/h = 2000 to 3000 ml per 24 hours = Bicarbonate-Alcaline-POLYURIA (BAP)
Avoid low Blood NaCl-levels = Salt Depletion. Therefore, NO LOW-SALT-DIET
MAINTENANCE of BAP: Continue intake of NaHCO3 until Optimum Kidney Function is reached and maintained according to the lowering of Serum-Creatinine. Use Minimum Diuretic-Dosis/24 hr
CONTROLS:
Depending on Clinical Condition e.g. Inpatient / Outpatient:
Blood-Gases, Serum-Electrolytes including Chloride !
Blood-Pressure: CAVE Hypotension. In Case of HYPER-Tension, lowering of RR !
Blood-Glucose: CAVE Hypoglycemia especially in Diabetics
URINE-Volumes: ml /12 h, ml /24h CAVE: Urine volumes up to 6000 ml/24 h are possible! Therefore:
Daily Control of BODY-WEIGHT, FLUID-BALANCE
URINE-pH-Testing: Use pH-Indicator-paper Range: pH 5,6 – 8.0 (Uralyt-UR MADAUS)
At best every time at Urine-passage. At least: 3 times daily !
Keep PATIENT-RECORD !
Results
In view of the the high 24 hour Urine-Output negative fluid-balance (if desired) may easily be achieved and will also permit full parenteral nutrition even with high I.V.- fluid volumes (6). Creatinine-decrement daily will be 1 to 2 mg/dl with respect to the general clinical condition of the patient, Age, preexixting renal damage, Cardio-Circulatory-Condition etc.
The total number of ARF-patients, who thus have been treated during the past 20 years cannot be given pricisely. The various Divisions where the patients belonged performed the Renal Resurrection Therapy on there own, after initial consultation with us. Seven Doctoral Theses about the use of BAP in ARF were written in various medical Departments of the Technical University of Munich (TUM). Two experimental animal studies on rats, using a gentamcin-toxic and an ischemic ARF-model also confirmed the efficacy of BAP-procedure to prevent ARF (3, 14).
Discussion
The basic patho-physiological efficacy of the Bicarbonate-Alcaline-Polyuria- regimen can be explaned is as follows:
The KIDNEY, after a renal insult which led to significant renal insufficiency, is unable to perform its three main tasks:
- The Kidney can no longer CONCENTRATE
- The Kidney can no longer DILUTE
- The Kindey can no longer ACIDIFY
The FETAL KIDNEY gradually develops these abilities to produce urine step by step until birth. Therefore, the ontogenetic development of the kidney to produce concentrated urine represents the abbreviated repetition of Phylogenesis. During the phase of Evolution, approximately 200 Million Years ago, the identical development of Kidney Organs took place in the first land-inhabitating mammals. They preserved their original External Environment within their circulation as their Internal Environment which enabled them to take the step from Sea-Water on to the dry land. (See Fig. 1). The principles of these fundamental physiological data can therefore still to date be applied clinically.
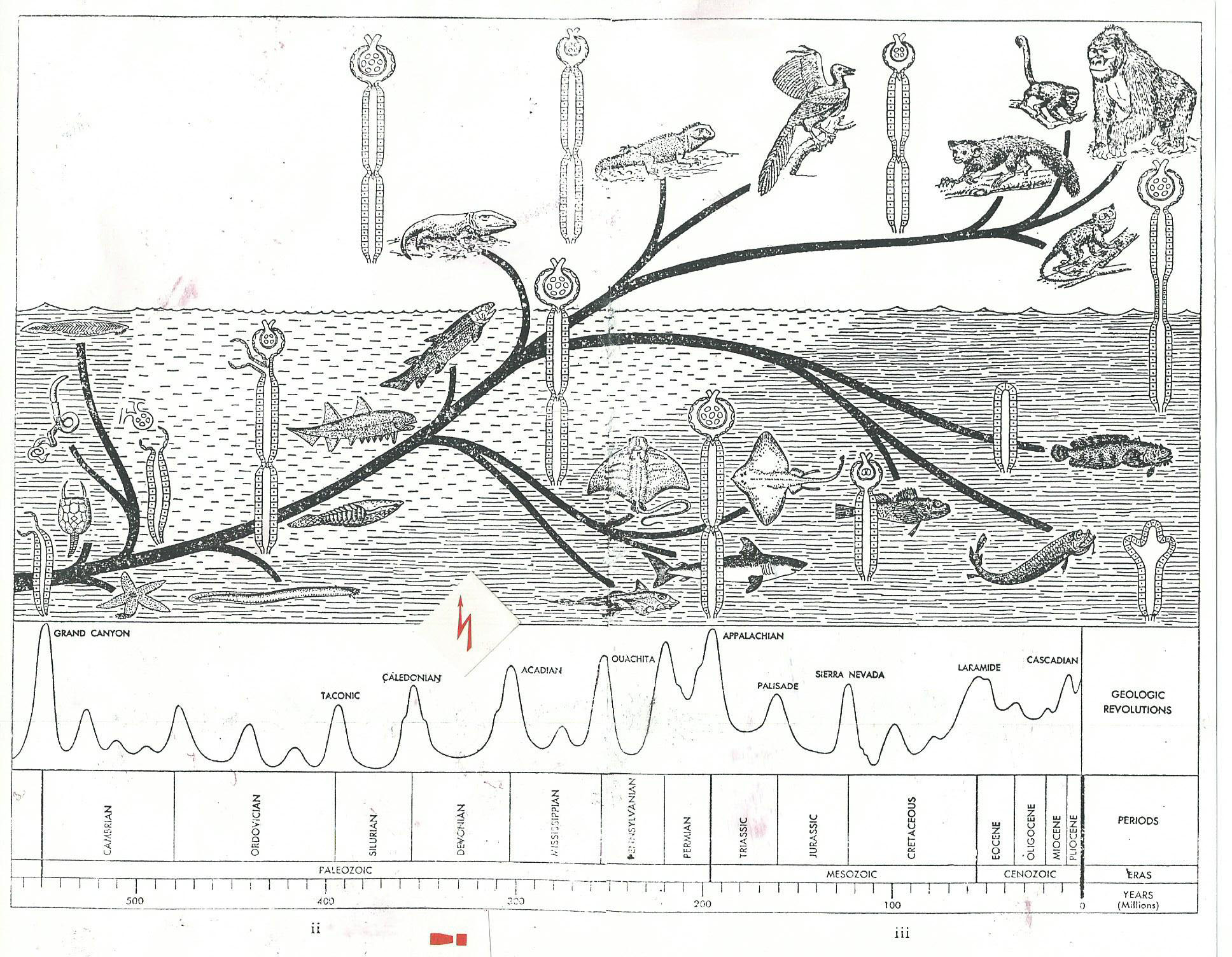
The “Kopp’s Solution”, is therefore identical to the composition of the Sea-Water at the time of DEVON-CARBON in which at that time Amphibia and early Mammals lived.
The physiological laws of renal function were described in the textbooks on the Physiology of the Kidney written by HOMER SMITH (22), ROBERT F. PITTS (17), KLAUS THURAU (25), JÜRGEN SCNERMANN (19), O. MATHISEN (15), ROBERT SCHRIER (20), R. GREGER (7) and many others.
Homer W. SMITH already described the important fact that in all mammals living on land the arterial blood supply of the Nephron is controlled and regulated by the Vas afferens and Vas efferens of the glomerulum. Thereby, the metabolic activity of the Nephron depends on and is warranted by the magnitude of the glomerular bloodflow.
Robert F. PITTS , based on his self-experiment, first described the principles of the renal excretion of bicarbonate, which depends on the constancy of tubular reabsorption of bicarbonate when the maximum concentration of bicarbonate in the blood exceeds 28 mMol/dl (See Fig 2 ).
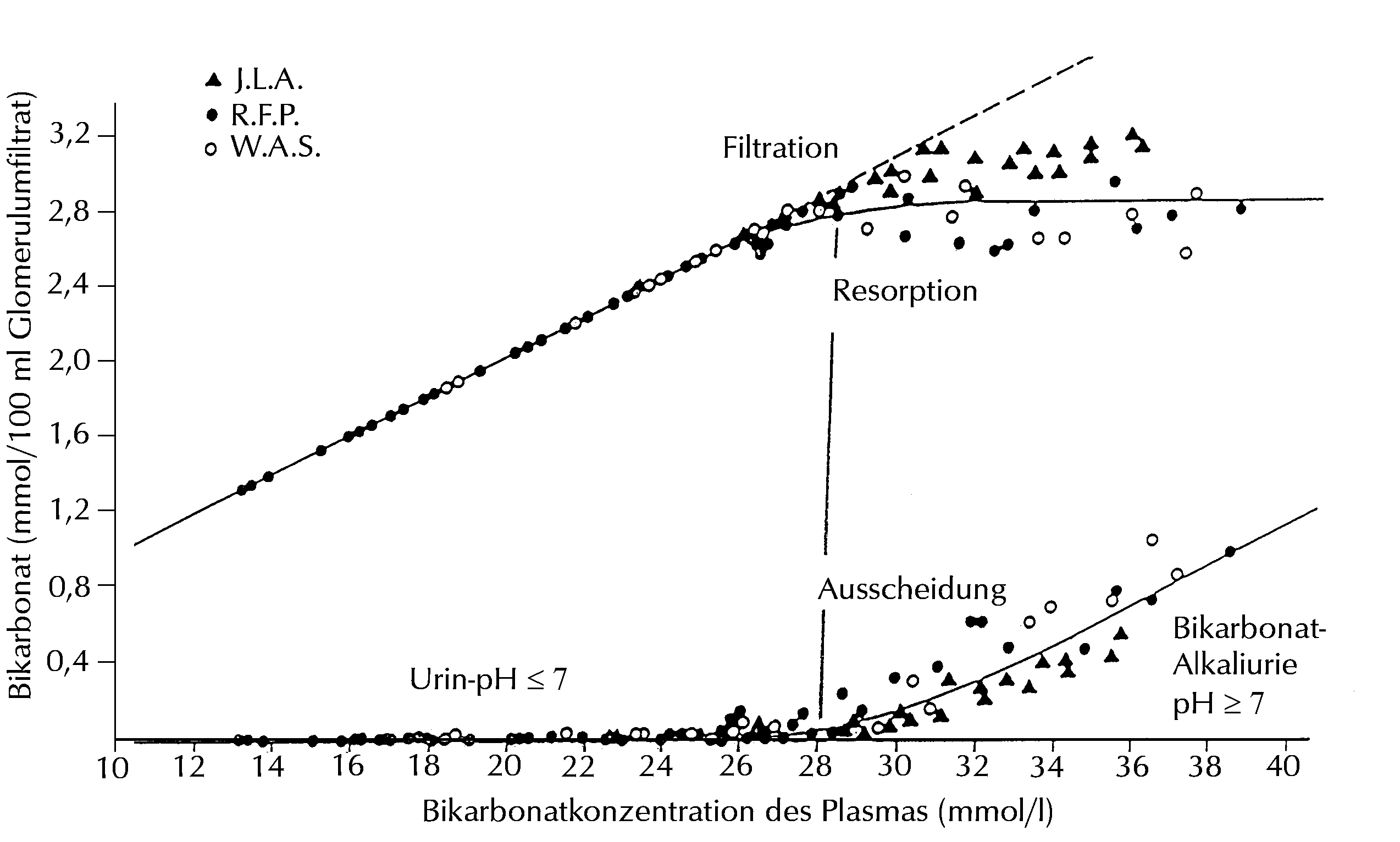
Filtration, reabsorption and excretion of bicarbonate as functions of plasma-concentration In normal man. (From Pitts, R.F.;
Ayer and Schiess, W.A.: J. Clin. Invest. 28:35, 1949), modified by K.F. Kopp: At bicarbonate- plasma-concentrations of
28 mmol/l and above (~ BE > 7) Bicarbonate-Alcaline-diuresis is present.
J. Schnermann and K. Thurau first described the regulation oft he Glomerul-Tubular-Balance (GTB) and of the Glomerular-Filtration-Rate (GFR) via Vasoconstiction or Vasodilation of the glomerular Vas Afferens and Vas Efferens.
J. Schnermann (19) discovered the unique vasodilating property of NAHCO3.
O. Mathisen et al. (15) were able to confirm, NAHCO3 to be the “KEY-MEDIATOR” of the Glomerulo-Tubular Balance (GTB).
R. Greger (7) described the energy-lowering effect of loop-diuretics in the Thin Ascending Loop (TAL) of the Kidney on the Na2 CL- K+ Cotransporter and the Enhancement of Diuresis due to this effect.
As a result, a new form of diuresis, namely the Bicarbonate-Alcaline-Polyuria (BAP) could be developed which up to now has been unknown. BAP eliminates most efficiently all uremic retention-products, endogenous and exogenous toxins, it also relieves Nephron-ischemia due to the vasodilating effect of NaHCO3. The so-called “Re-trafficking” of nephrotoxic substances is efficiently reduced and thereby provides the nephro-protective effect of BAP (1).
The clinical combination of all these synergistic effects led to the clinical protocol of the Bicarbonate-Alcaline-Polyuria (BAP) regimen, as a prerequisite to produce extremely efficacious renal diuresis and urinary volumes so far unknown . The prophylactic use in incipient ARF is therefore most promising.
Normally, the glomerular filtrate is reabsorbed in the proximal tubule up to 70 %. In the case of supersaturation of the glomerular filtrate with bicarbonate, the excessive bicarbonate, together with its filtrate will not be reabsorbed and an increased filtered flow thereby reaches the distal tubules and the collecting duct to be excreted in polyuric urine- volumes including all uremic waste-products. This explaines the efficient elimination of uremic toxins by BAP.
Various controlled studies did show that the application of diuretics in various amounts and its combination with the infusion of electrolyte-solutions produced Polyuria, but this type of enhanced diuresis was not able to lower or to inhibit the retention of uremic substances neither in ARF nor in CRF. However, clinical attempts with failing results are still being made worldwide (4, 21).
Figure 3 and Fig 4 demonstrate the principle of the Bicarbonate-Alcaline-Polyuria (BAP)-regimen. In Fig 3 the situation of Oligo-Anuria which is hardly influenced by Furosemide is represented. Fig 4 shows the contrasting effect of Bicarbonate to produce Polyuria.
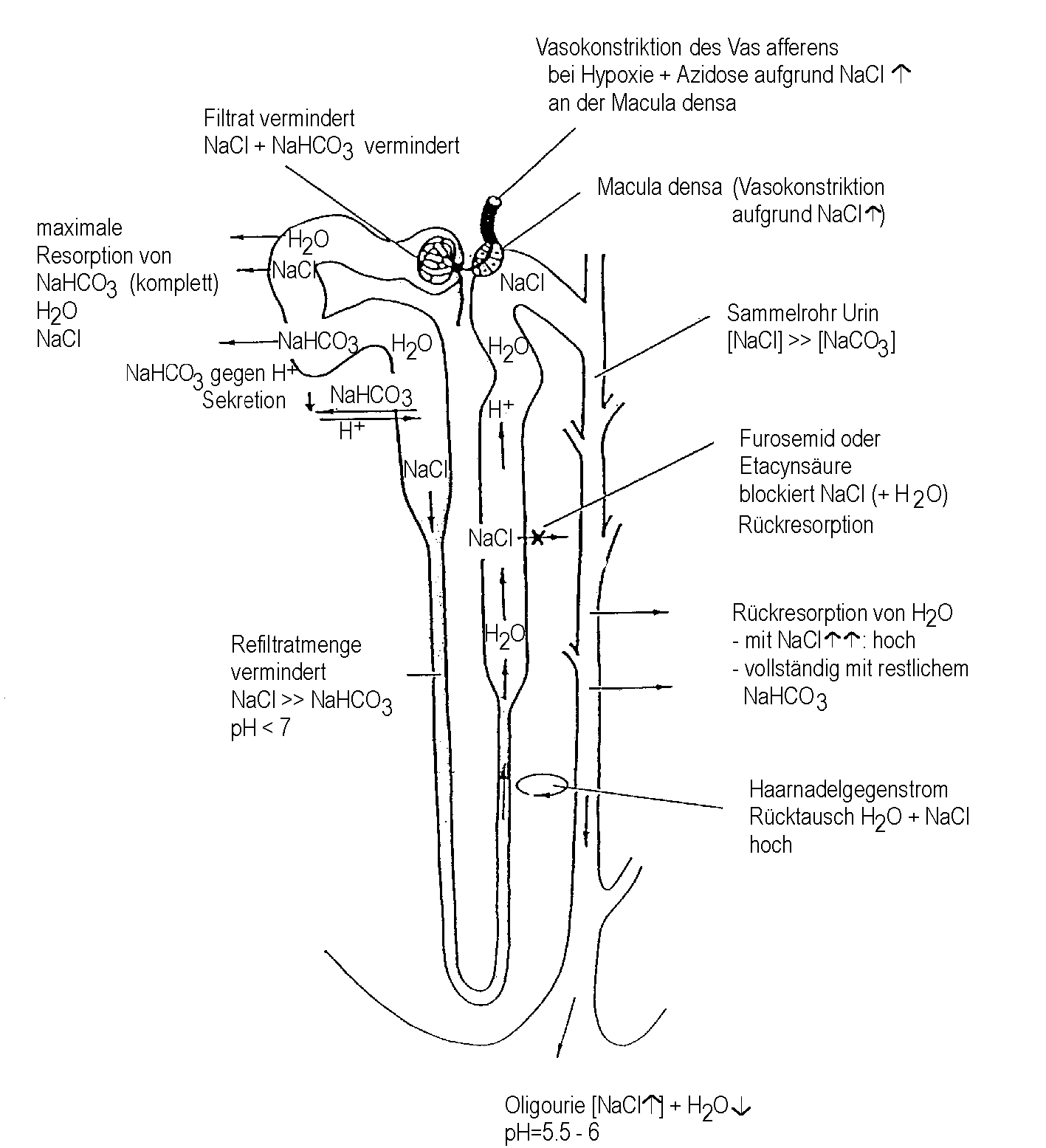
Salt-Water-Diuresis at pH < 6 + Loop-Diuretic resulting only in a moderate diuresis of Salt and Water (Oliguria)
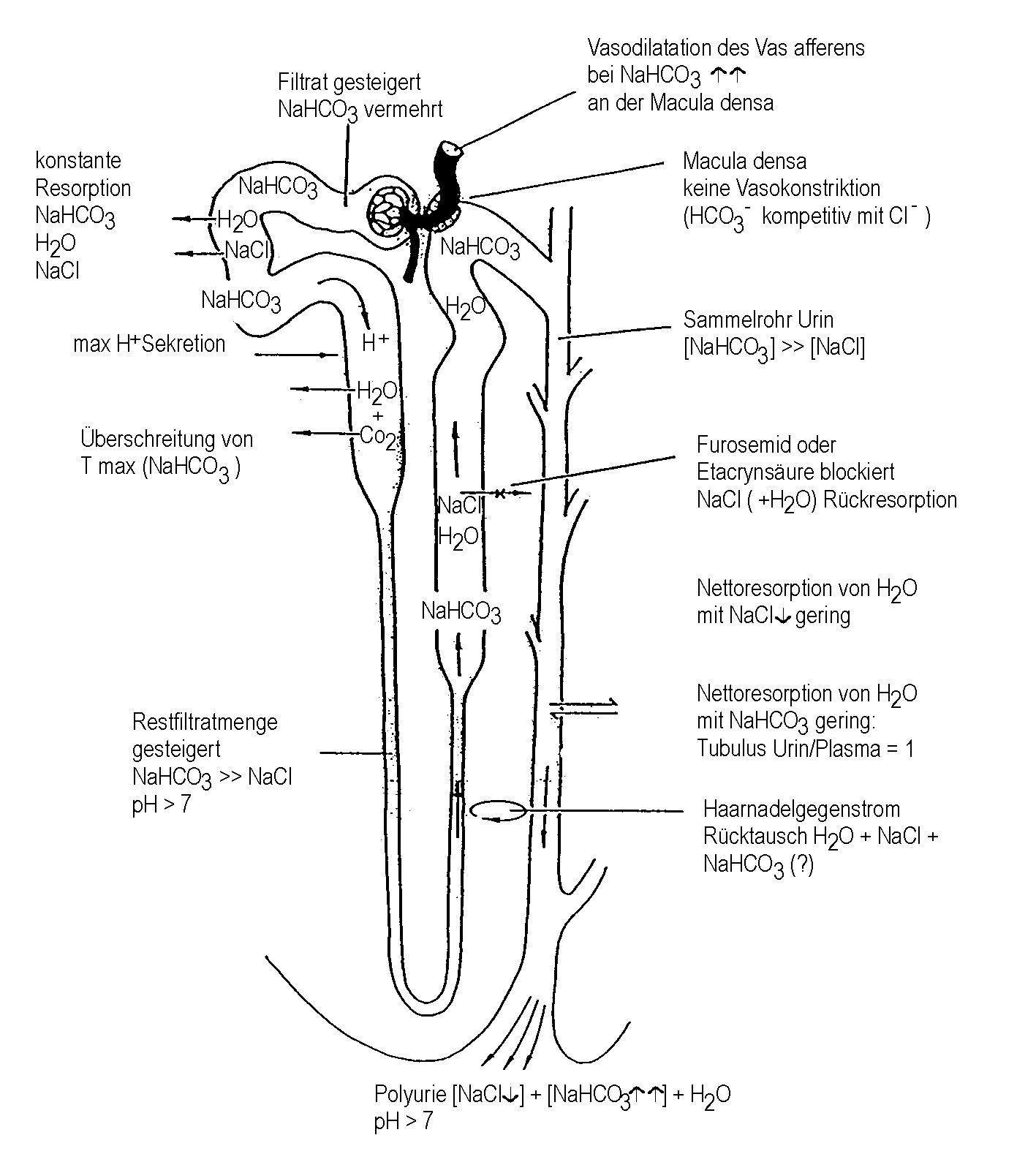
Tubular transport conditions together with an enhanced glomerular flowrate eventually result in Bicarbonate-Alcaline-Polyuria; pH > 7.0
Summary
The routine use of the Bicarbonate-Alcaline-Polyuria (BAP) protocol for the conservative Prophylaxis and Therapy of ARF of all 10 RISK-Groups mentioned before, will lead to
- a significantly reduced number of cases in need of Acute Dialysis for ARF,
- a significantly greater number of surviving patients due to the conservative management of ARF
- a significantly greater number of vital and polyuric Kidneys suitable for TRANSPLANTATION
Literature
- Abbate, M. et al. (1999). Nephrotoxicity of increased glomerular protein traffic. Nephrol Dial Transplant 14: 304 – 312.
- Anderson, R.J. et al. (1999). Renal failure predisposes patients to adverse outcome after coronary artery bypass surgery. K. I.: 55, 1057 – 1062
- Blasberg, A., Kopp, K.F. (1999). Die Wirkung einer Bikarbonat-Alkali-Polyurie auf das Gentamycin-induzierte akute Nierenversagen der Ratte. Diss., Inst. f. Exper. Chirurgie, TUM, München, BRD.
- Brown, C.B., Ogg, C.S., Cameron, J.S. (1981). High dose furosemide in acute renal failure: a control trial. Clin. Nephr. 15, (2) 90 – 96.
- Douma, C.E. et al. (1997). Predicting mortality in intensive care patients with acute renal failure treated with dialysis. Am Soc Nephrol 8: 111 –117.
- Garella, S., Chang, B.S., Kahn, S.I. (1975). Dilation acidosis and contraction alkalosis: Review of a concept. Ki 8, 279 - 283.
- Greger, R. (1999). New insights into the molecular mechanism of the action of diuretics. Nephrol Dial Transplant 14: 536 – 540
- ICN XVth, Sat. Symp. (1999). Acute Renal Failure, Santiago –Chile May 7 & 8.
- Kopp, K.F., Müller, Thul. G. (1981). Prophylaxis and emergency treatment of acute renal failure by acute intravenous bicarbonate loading in Acute Renal Failure. H. E. Eliahou Ed. Proc. Sat. Symp. 8th ISN meeting.
- Kopp, K.F. (1993). Das akute Nierenversagen ANV. Intensiv 1: 17 – 19.
- Kopp, K.F. (1976). Diagnostik und Therapie von Nierenfunktionsstörungen beim Schwerverletzten. Unfallmedizinische Tagung der Landesverbände der gewerblichen Berufsgenossenschaften 28, 107 – 114.
- Liaño, F., Gallego, A., Pasqual, J., Garcia-Martin, F., Teruel, J.L., Marcen, R., Orofino, L., Orte, L., Rivera, M., Gallego, N., Quereda, C., Ortuño, J. (1993). Prognosis of acute tubular necrosis: An extended propectively contrasted study. Nephron 63:21-31.
- Liaño, F. (1994). Severity of acute renal failure: the need of measurement. Nephrol. Dial. Transplant 9 [Suppl.4]: 229 – 238.
- Lücke, D., Kopp, K.F. (1999). Die Wirkung einer Bikarbonat-Alkali-Polyurie auf das ischämisch induzierte akute Nierenversagen bei der Ratte. Diss., Inst. f. Exper. Chirurgie, TUM, München, BRD.
- Mathisen, Ø., Monclair, T., Holdaas, H., Kiil, F. (1978). Bicarbonate as Mediator of proximal tubular NaCL reabsorption and Glomerulotubular Balance. Scand. Clin. Lab. Invest. 38,7: pp. 7-17.
- Palmer, B.F., Alpern, R.J. (1997). Metabolic Alkalosis . J. Am. Soc. Nephrol., pp. 1482-146.
- Pitts, R.F. (1974). Physiology of the Kidney and Body Fluids. Third Ed. Year Book Med. Publ., LCCC No. 23-94395.
- Sanderson, P.H. (1978). "Alkalosis": a medical muddle. J. Roy. Coll. Phycns. 12: 201-209.
- Schnermann, J. (1975). Regulation of single nephron filtration rate by feedback – facts and theories. Clin. Nephrol. Vol. 3, pp.75 – 81.
- Schrier, R.W., Burke, T.J., Conger, J.D., Arnold, P.E. (1981). Newer aspects of acute renal failure. Proc. 8th Int. Congress Nephrol., Athens p. 63 – 69.
- Shilliday, R., Quinn, K.J., Allison, M.E.M. (1997). Loop diuretics in the management of acute renal failure: a prospective, double-blind, placebo-controlled, randomized study. Nephrol Dial Transplant 12: 2592-2596.
- Smith, H.W. (1959). From Fish to Philosopher. The Story of Our Internal Environment. Ciba Edition, Library of Congress Cat. Card No. 53-7332.
- Star, R.A. (1998). Treatment of acute renal failure K.I. Vol 54, pp. 1817-1831
- Thadhani, R., Pasqual, M., Bonventre, J.V. Acute renal failure N.E.J.M. Vol 334, No. 22 p. 1448 – 1460.
- Thurau, K., Boylan, J.W. (1976). Acute Renal Success, the unexpected logic of oliguria in acute renal failure. A. J. Med. Vol. 61. P. 308-315.